ALIF Surgery: Anterior Lumbar Interbody Fusion
Summary: Anterior lumbar interbody fusion (ALIF) is a spinal fusion procedure that uses a frontal (anterior) approach to access the lumbar (lower) spine. It is commonly used to treat degenerative disc disease, spondylolisthesis, and other causes of low back pain. This article explains who may benefit from ALIF surgery and provides details on the procedure, recovery, potential risks, and success rates.

In this article
- What is ALIF surgery?
- What conditions does it treat?
- Who is a good candidate?
- Why ALIF instead of a PLIF, LLIF or TLIF?
- What tests or scans will I need?
- How is it performed?
- What type of anesthesia is used?
- Is ALIF minimally invasive?
- How painful is ALIF surgery?
- How long does ALIF surgery take?
- How long will I be in the hospital?
- What is the recovery time?
- What activities should I avoid after ALIF?
- Will I need physical therapy?
- How soon can you walk after an ALIF surgery?
- How big will my ALIF scar be?
- What are the risks?
- Will I lose flexibility in my spine?
- How successful is ALIF surgery?
- Key takeaways
What is ALIF surgery?
Anterior lumbar interbody fusion (ALIF) is a spinal fusion procedure in which surgeons navigate through the abdomen to access the front of the spine and fuse two or more vertebrae in the lower back together. The procedure involves an “approach” surgeon (who provides access to the spine) and a spine surgeon, working together.
Anatomy of the lumbar spine
The lumbar portion of the spine contains the five spinal vertebrae (L1 to L5) of the lower back.
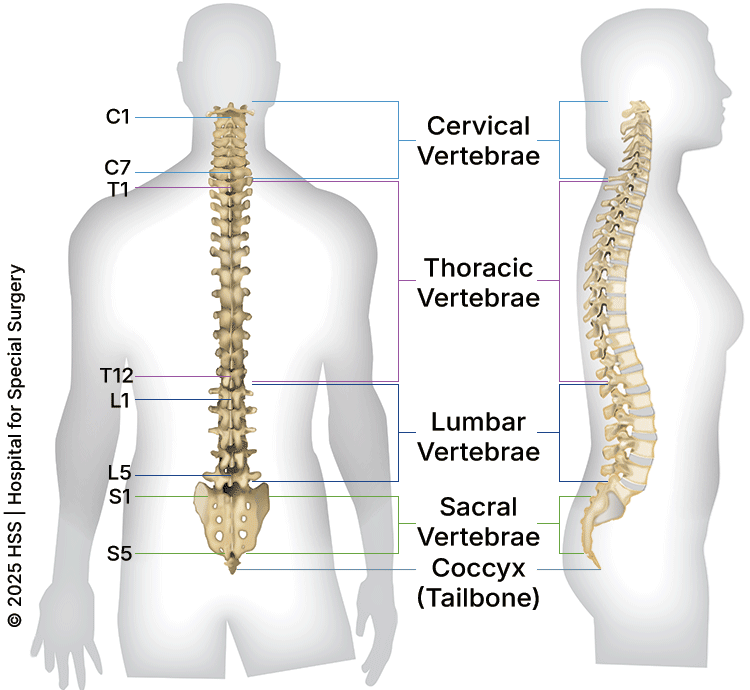
Illustration of cross-section of spine, dorsal (back to front) and lateral (side) views, showing its vertebral sections.
In addition to the lumbar vertebrae, an ALIF procedure may sometimes also involve the intervertebral disc located between the L5 vertebra and the highest vertebra (S1) of the sacral spine that includes the sacrum and coccyx (tailbone). This is known as an L5/S1 ALIF procedure.
What conditions does ALIF surgery treat?
The best way to think about ALIF surgery is that it is used to restore the vertical space between two spinal vertebrae, fusing them as a result. When a lumbar disc degenerates, the space between the two vertebrae it nests between is compromised. This can lead to a pinched nerve, instability, arthritis or spinal deformity. Thus, ALIF can be used to treat degenerative disc disease, spondylosis (spinal arthritis), spondylolisthesis (instability), and spinal deformities such as degenerative scoliosis.
Who is a good candidate for ALIF surgery?
The best candidates for ALIF surgery are people experiencing disc collapse at the lowest lumbar segments of the spine (L4/5 and L5/S1) who need the maximum restoration of height in that disc space to relieve the cause of their pain.
While it is possible to perform ALIF at upper lumbar levels (L1/2, L2/3, L3/4), it is often more challenging due to the anatomy in this region. When a restoration of disc space is needed at upper lumbar levels (L1/2, L2/3, L3/4), lateral lumbar interbody fusion (LLIF) or transforaminal lumbar interbody fusion (TLIF) are usually better options.
Why is ALIF done instead of other types of spinal fusion (like PLIF or TLIF)?
The way to think about spinal fusion is that fusions can occur through two places: the disc space between vertebrae (“interbody fusion”) or the posterior bones of the spine (“posterolateral fusion”). Surgeons can access the disc space in three ways. Through the:
- Back (“posterior”) as in PLIF or TLIF procedure.
- Side (“lateral”) as in an LLIF or OLIF procedure.
- Front (“anterior”) as in the ALIF procedure.
The decision to use one approach versus another usually depends on several factors, including:
- Which spine level(s) need to be addressed.
- The patient’s specific anatomy, bone quality, and flexibility of the disc space.
- Any history of previous surgeries.
- Surgeon preference.
What tests or scans will I need before surgery?
At a minimum, most patients will need X-rays and MRI. MRI is used to visualize the nerves. CT myelograms can also assess the nerves, and can be performed for patients who cannot get an MRI (for example, they may have a pacemaker or spinal cord stimulator incompatible with MRI machines).
Standard CT scans are often used as well to assess bony anatomy. At HSS, we also believe that nearly every patient above a certain age should have bone quality assessed before spinal fusion. This can be done with a specialized CT scan, (Quantitative CT, “QCT”) or a standard DEXA bone scan.
How is ALIF surgery performed?
Spelling out the acronym – "anterior lumbar interbody fusion" – provides language to describe how the procedure is performed. There are two major parts to ALIF surgery:
- The surgical approach: This is performed by a surgeon with expertise in abdominal or vascular surgery, who creates an anterior (frontal) opening to access the lumbar spine.
- The discectomy and interbody fusion: This is performed by the spine surgeon. It involves removing the spinal disc and replacing it with an interbody device between the vertebrae (also called "vertebral bodies") to fuse them: In other words, interbody fusion.
Surgical approach
The approach begins with a horizontal or vertical incision on the abdomen. Next, the approach surgeon splits the abdominal muscles and moves the abdominal contents (contained in a covering called the “peritoneum”) to the side. This allows them to visualize the front of the spine, during which they assess the relationship between the spine and major blood vessels (the vena cava, aorta, and common iliac arteries and veins). These vessels supply blood to the legs. Once these vessels are protected with a retractor, the spine surgeon comes in to perform the second part of the surgery.
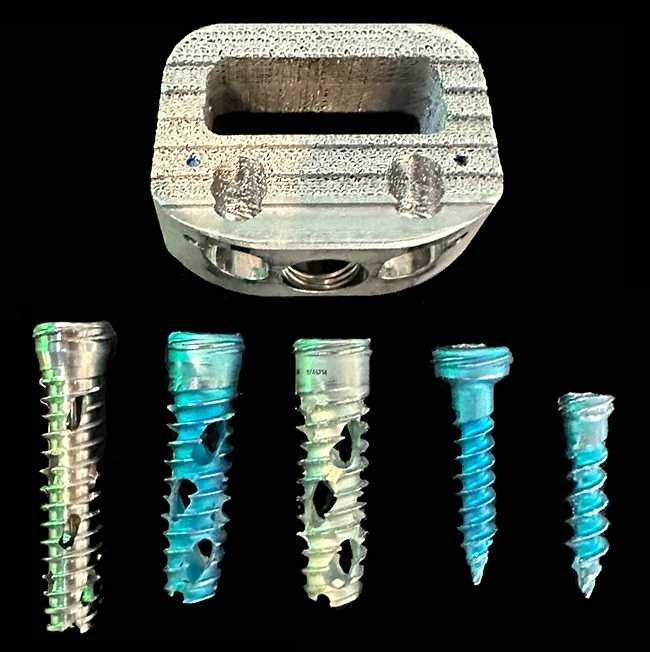
Discectomy and interbody fusion
The second part of the ALIF is performed by the spine surgeon. In this part of the procedure, the disc is removed from the spine (discectomy), working in an anterior-to-posterior (front-to-back) direction. Sometimes, if there is a substantial bony deformity or spondylolisthesis, part of the front portion of vertebrae will have to be removed as well. An interbody device (often called a “cage” or “spacer”) is then placed into the empty space where the disc was. This cage is often filled with bone grafting materials. Screws are sometimes placed through the cage to secure it in place.
If the surgeon feels that extra fixation is needed to further stabilize the vertebrae, the incision in the front will be closed and the patient will then be flipped over in order to place posterior screws and rods into the vertebrae (meaning that this instrumentation is inserted from the back toward the front of the spine).
Animation: ALIF spinal fusion surgery
This video provides an illustrated look at the ALIF procedure, which makes space between the vertebral bodies to relieve pressure and create more room for nerves to exit the spinal column.
What type of anesthesia is used?
General anesthesia – this means the patient must be intubated.
Is ALIF minimally invasive?
Anterior lumbar interbody fusion (ALIF) is considered a minimally invasive surgery as it uses anatomical corridors (surgical access routes) that take advantage of normal tissue planes, meaning the spaces between muscles, nerves, organs or other soft tissues.
How painful is ALIF surgery?
Given that ALIF does not involve disruption of the posterior muscles that cover the spine, the surgery is usually better tolerated than a posterior lumbar fusion. About 1 in 3 patients will develop pains in the legs, sometimes accompanied by weakness in the ankle or great toe – this is due to changing the environment around the nerve. Generally, these pains resolve after 3 months.1
How long does ALIF surgery take?
The length of an ALIF surgery is extremely variable as it is highly dependent on each patient’s individual anatomy. For people having an L5/S1 ALIF with anatomy that allows for easy access to the front of the spine, the procedure can take one to two hours from start to finish. For patients with prior surgeries, spinal deformities, or anatomy that makes it difficult to access the spine, the surgery can take much longer.
If the patient requires a “flip” in order to place posterior screws and rods, this also adds to the amount of time required for the surgery.
How long will I be in the hospital after ALIF surgery?
For a simple one-level ALIF, with or without posterior screws, many patients will leave the next day after surgery. Making predictions for length of stay after multilevel fusions becomes more difficult.
Rather than the surgery itself, the hospital length of stay usually depends more on the patient’s preoperative health, their discharge plan (whether they will go straight home from the hospital or to a rehabilitation facility) and their ability to respond to anesthesia. (For example, some patients have a difficult time getting normal urination or bowel function back after anesthesia which can prolong the hospital course.)
The best things a person having ALIF surgery can do are to recognize that hospital length of stay after spine surgery can be variable and to follow the recommendations of the inpatient team about when they will be ready to leave the hospital.
What is the recovery time for ALIF surgery?
At HSS, we like ALIF patients to get up and begin physical therapy on the day of their procedure, and to try “living their life normally” as soon as they can upon getting home.
However, most patients should take it easy for the first 2 to 4 weeks after surgery: resting, doing short walks, and avoiding lifting. The specifics of activity and recovery should be discussed with their surgeon. Patients are generally prevented from engaging in high-impact activities – such as running, weightlifting, sports (including golf) – until the fusion between the vertebrae is more mature (around 3 to 6 months).
Importantly, if an ALIF is performed as part of a larger procedure (such as a deformity correction or multilevel anterior/posterior fusion), the hospital stay can be much longer. This adds substantial variability to the recovery time.
What activities should I avoid after ALIF surgery?
Nearly all HSS surgeons will recommend a several-week period of avoiding deep bending through the back, excessive twisting through the back, and lifting more than a certain weight – usually 5 to 20 lbs. (2.5 to 9 kg) after ALIF. The length of time that activities are restricted is based on the individual surgeon.
Do you need physical therapy after an ALIF surgery?
The need for physical therapy is highly dependent on surgeon preference, the patient’s preoperative fitness, and individual recovery course. Some patients may not need physical therapy at all, while others may need many sessions.
How soon can you walk after an ALIF surgery?
At HSS, we try to get our patients walking on the day of an ALIF surgery.
How big will my ALIF scar be?
ALIF scars are very similar to scars from C-sections. The incision length for an ALIF is dependent on the number of vertebral levels that need to be addressed and the patient’s frame and body type.
In terms of healing, everyone’s skin heals differently. For example, if your body generally forms thick scars, you are more likely than some others to form a thick scar after any surgery. Keeping your surgical incision out of the sunlight for the first year after surgery and using silicone strips can help improve scarring.
What risks or complications can occur with ALIF surgery?
There is generally a low rate of complication after ALIF surgery. Reviews of the spine literature show that the most common complications are ileus (2%), wound infection* (1%), retrograde ejaculation** (permanent in approximately 1%), and neurologic problems leading to leg pain, numbness, or weakness (1% or 2%). Less common complications include injury to the ureters or bowel.
However, the most serious risk of ALIF surgery is injury to the major blood vessels in front of the spine. Blood vessels are injured in approximately 1% to 2% of cases. Most of the time, these injuries are minor, and the approach surgeon repairs the vessel at the time of surgery. In the worst-case scenario, serious or unrepairable injuries to the major blood vessels can lead to loss of limb or even death.
Regarding longer-term complications, failure to heal (pseudarthrosis), hardware failure, or settling of the cage into the vertebral body (a condition known as “subsidence”) can occur and sometimes necessitate a second surgery.
*Some people are at higher risk of surgical site infections, such as those who are obese, undergo dialysis, or who are taking long-term corticosteroids.
**Retrograde ejaculation is when semen enters the bladder rather than exiting the penis, which can cause fertility complications in men.
Will I lose flexibility in my spine after ALIF?
Technically, you will have less flexibility in your spine after an ALIF. This is generally not noticeable for everyday activities or even most sports. Also, if a disc is already severely degenerated, it usually does not have much motion anyways. In such cases, fusing it may have no negative flexibility impact at all.
How successful is ALIF surgery?
The majority of studies show that anterior lumbar interbody fusion (ALIF) leads to a successful fusion between the vertebrae in at least 90% of cases, with many studies showing rates of fusion in greater than 95% of cases.
With regard to the success of the surgery in relieving preoperative symptoms, this is highly dependent on the reasons for having the surgery. Patients should speak with their surgeon about their particular case.
Key takeaways
- ALIF accesses the spine through the front of the abdomen, which eliminates the disruption of back muscles.
- It is best suited for restoring disc height and obtaining fusion in the lower lumbar spine (L4/5 and L5/S1).
- For a one to two level ALIF, most patients walk the same day and return home within three days.
- Complication rates are low but can include blood vessel injury or new weakness.
- Success rates exceed 90% in most cases.
Why choose HSS for lumbar decompression and fusion surgery?
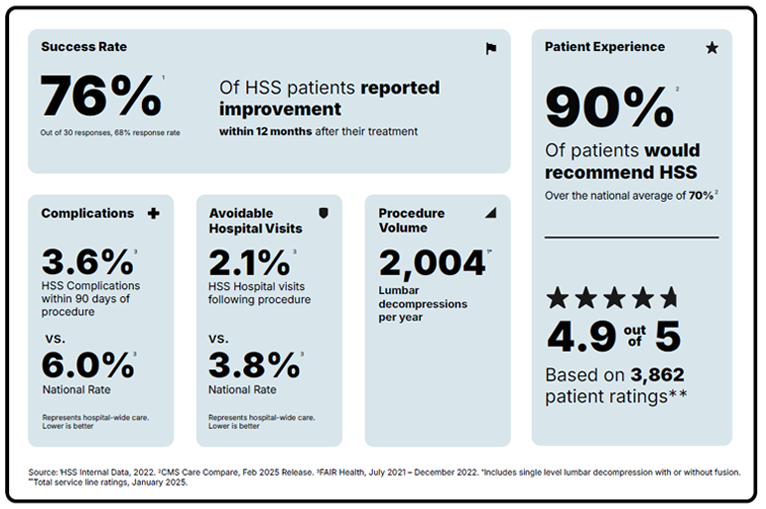
Lumbar spinal decompression with fusion is a surgery focused on reducing pain and getting you back to the activities you love. But not all hospitals achieve the same results. Some are more reliable than others. With the help of the HSS Hospital Reliability Scorecard, you can make sure you're asking the critical questions to find the hospital that's right for you. Understanding these data points will help you make the best decision for your care: See hospital reliability data
Authors
Explore Related Patient Stories
View All Patient Stories
Denis Ambio
Bushkill, PA
ALIF Surgery: Anterior Lumbar Interbody Fusion

Simone Lombardo
Wallkill, NY
ALIF Surgery: Anterior Lumbar Interbody Fusion

Glenn Emanuel
Scarsdale, NY
ALIF Surgery: Anterior Lumbar Interbody Fusion

Michael Centanni
Wall, NJ
ALIF Surgery: Anterior Lumbar Interbody Fusion

Rachel Kniewel
Ringwood, NJ
ALIF Surgery: Anterior Lumbar Interbody Fusion
References
- Araghi K, Fourman MS, Merrill RK, Maayan O, Zhao E, Pajak A, Subramanian T, Kim DN, Kamil R, Shahi P, Sheha ED, Dowdell JE, Iyer S, Qureshi SA. Postoperative Radiculitis After L5-S1 Anterior Lumbar Interbody Fusion. Spine (Phila Pa 1976). 2023 Sep 15;48(18):1317-1325. doi: 10.1097/BRS.0000000000004740. Epub 2023 Jun 1. PMID: 37259185. https://pubmed.ncbi.nlm.nih.gov/37259185/
- Body AM, Plummer ZJ, Krueger BM, Virojanapa J, Nasser R, Cheng JS, Prestigiacomo CJ. Retrograde ejaculation following anterior lumbar surgery: a systematic review and pooled analysis. J Neurosurg Spine. 2021 Jul 16;35(4):427-436. doi: 10.3171/2020.12.SPINE201101. PMID: 34271542. https://pubmed.ncbi.nlm.nih.gov/34271542/
- Kazarian GS, Du J, Gang CH, Shahi P, Asada T, Lu A, Korsun M, Tuma O, Singh N, Araghi K, Maayan O, Singh S, Iyer S. Preoperative and Postoperative Segmental and Overall Range of Motion in Patients Undergoing Lumbar Spinal Fusion Using HA-Infused PEEK and HA-Treated Titanium Alloy Interbody Cages. Global Spine J. 2025 Mar;15(2):1077-1086. doi: 10.1177/21925682231223117. Epub 2023 Dec 20. PMID: 38116633; PMCID: PMC11877480. https://pubmed.ncbi.nlm.nih.gov/38116633/
- Lee D, Lee R, Weinreb J, Chalif E, Mohile N, Heyer JH, O'Brien J. Risk Factors for Surgical Site Infections After Single-Level Anterior Lumbar Interbody Fusion. Surg Infect (Larchmt). 2023 Aug;24(6):514-521. doi: 10.1089/sur.2023.070. Epub 2023 Jun 15. PMID: 37327050. https://pubmed.ncbi.nlm.nih.gov/37327050/
- Phan K, Xu J, Scherman DB, Rao PJ, Mobbs RJ. Anterior Lumbar Interbody Fusion With and Without an "Access Surgeon": A Systematic Review and Meta-analysis. Spine (Phila Pa 1976). 2017 May 15;42(10):E592-E601. doi: 10.1097/BRS.0000000000001905. PMID: 27669042. https://pubmed.ncbi.nlm.nih.gov/27669042/