Knee Arthroscopy
Medically reviewed by Frank A. Cordasco, MD, MS
Summary: This article provides an overview of arthroscopic knee surgery. It explains why it is usually preferred to performing open knee surgery and which surgical procedures are commonly performed using this method. Readers will learn the advantages of arthroscopy for both diagnosing and treating various knee conditions, how the procedure works, what type of anesthesia is typically used, and recovery expectations.

What is knee arthroscopy?
Knee arthroscopy is a minimally invasive technique that allows orthopedic surgeons to assess – and in most cases, surgically treat – a range of conditions affecting the knee joint. In particular, it is commonly used for ACL reconstruction and meniscus surgery.
Arthroscopic surgery in the knee takes place only after the immediate post-injury swelling and inflammation have diminished, and the patient has recovered almost complete range of motion.
What knee surgeries are performed arthroscopically?
ACL reconstruction and trimming or repair of a torn meniscus in particular are among the most commonly performed arthroscopic surgeries – often done at the same time.
Other knee surgeries often performed arthroscopically include:
- reconstruction of other knee ligaments, such as the MCL and PCL
- synovectomy
- articular cartilage repair and regeneration
- smoothing out defects in or extracting small pieces of loose cartilage or soft tissue inside an arthritic knee joint
Arthroscopy can also help in the treatment of knee fractures in combination with an open procedure to repair the bone. When a patient has a broken knee, arthroscopy allows surgeons to see the area without disrupting the joint. They can set the bone and place any necessary pins, screws, or additional hardware with minimal risk of additional injury to the patient.
Combined arthroscopic ACL and meniscus surgery
Tears of the ACL and the meniscus are both common, particularly in athletes. These injuries often occur in conjunction with one another, and so surgeons often perform arthoscopic ACL surgery and meniscus surgery at the same time. These combined injuries can happen concurrently amid the same traumatic event, but they can also occur sequence, where a person first tears their ACL, and then later tears their meniscus, which becomes more vulnerable due to the resulting instability in the knee.
More than 60% of patients diagnosed with an ACL tear also have a meniscus tear. A gender-specific difference in ACL injuries among young female athletes has been demonstrated in recent years. Females are 2 to 6 times more likely to tear their ACL than their male counterparts, depending upon the sport.3
Some ACL and meniscus injuries can be treated nonsurgically with rest, physical therapy, and activity modification. However, in an active young person, forgoing ACL reconstruction or meniscus repair is likely to result in persistent instability and pain in the knee, as well as setting the stage for degenerative arthritis if they are unwilling to modify their sport-related activities significantly.
What are the advantages of arthroscopic knee surgery?
The primary advantage of arthroscopy is that it eliminates the need for large incisions and facilitates multiple views inside the joint, usually with little damage to surrounding soft tissues. Before arthroscopy was available, an open surgery called an arthrotomy and surgical dislocation of the patella (knee cap) was required to diagnose some knee conditions.
While most orthopedic surgeons continue to rely on X-rays and MRI to provide important preliminary information about a knee injury, many agree that arthroscopy is the best diagnostic tool available. It offers pieces of information that the other tests don't. MRI is a wonderful tool to evaluate the structure of the soft tissues of the knee. But a surgeon can learn much more about an injury by viewing it directly through a scope and physically probing the soft tissues. Imaging alone does not provide tactile information sometimes required to make some diagnoses.
How does knee arthroscopy work?
During the procedure, the orthopedic surgeon makes small incisions or portals in the affected joint, and then inserts a tiny camera and fiber optics to light the interior space. Pictures obtained with the camera are then projected onto a screen in the operating suite.
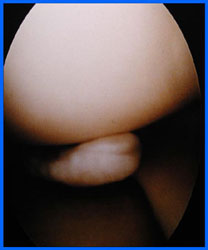
Arthroscopic photo of a meniscus tear.
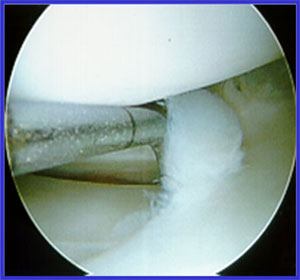
Arthroscopic photo of meniscus tear trimming.
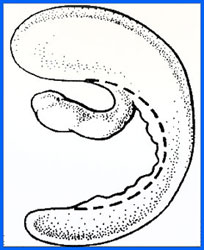
Illustration showing the location of trimming.
Is knee arthroscopy outpatient?
Generally, yes. Most patients go home the same day of surgery.
What kind of anesthesia is used in knee arthroscopy?
At HSS, arthroscopic surgery of the knee is generally performed with regional anesthesia or, occasionally, local anesthesia. General anesthesia is rarely indicated.2
What is the recovery process for knee arthroscopy?
Recovery time varies widely by procedure and the extent of a person's injury. For a competitive athlete undergoing ACL reconstruction, a period from about 6 to 9 months is an average time required before they can return safely to collision sports. During that period the patient will participate in a rehabilitation program designed to restore range of motion, strengthen muscles, and regain balance and sports-specific skills.
How to choose an orthopedic surgeon for knee arthroscopy
If you are considering an arthroscopic procedure, it's important to be sure that the orthopedist is qualified. Most orthopedic surgeons have the appropriate training to perform diagnostic arthroscopy, meaning the use of the technique to evaluate the knee and diagnose injuries and conditions. However, orthopedic operations such as ligament reconstructions, meniscus repairs, meniscal allograft transplantations, and articular cartilage restoration techniques, require specialized training in sports medicine or arthroscopic surgery.
Key takeaways
- Knee arthroscopy is a minimally invasive technique commonly used to diagnose and treat knee conditions such as ACL tears, meniscus injuries and cartilage damage.
- Arthroscopy allows surgeons to see and probe the knee joint directly, often providing more precise diagnostic information than imaging alone.
- Recovery varies by procedure. A professional athlete undergoing ACL reconstruction typically requires 6 to 9 months of structured rehabilitation before returning to full activity.
- Successful outcomes depend in part on choosing an orthopedic surgeon with specialized training in arthroscopic and sports medicine procedures.
References
- Battaglia MJ 2nd, Cordasco FA, Hannafin JA, Rodeo SA, O'Brien SJ, Altchek DW, Cavanaugh J, Wickiewicz TL, Warren RF. Results of revision anterior cruciate ligament surgery. Am J Sports Med. 2007 Dec;35(12):2057-66. doi: 10.1177/0363546507307391. Epub 2007 Oct 11. PMID: 17932401. https://pubmed.ncbi.nlm.nih.gov/17932401/
- Dunn WR, Cordasco FA, Flynn E, Jules K, Gordon M, Liguori G. A prospective randomized comparison of spinal anesthesia versus local anesthesia with propofol infusion for knee arthroscopy. Arthroscopy. 2006;22(5):479-83. PMID: 16651155. https://pubmed.ncbi.nlm.nih.gov/16651155/
- Toth AP, Cordasco FA. Anterior cruciate ligament injuries in the female athlete. J Gend Specif Med. 2001;4(4):25-34. PMID: 11727468. https://pubmed.ncbi.nlm.nih.gov/11727468/
- Williams RJ 3rd, Warner KK, Petrigliano FA, Potter HG, Hatch J, Cordasco FA. MRI evaluation of isolated arthroscopic partial meniscectomy patients at a minimum five-year follow-up. HSS J. 2007 Feb;3(1):35-43. doi: 10.1007/s11420-006-9031-2. PMID: 18751768; PMCID: PMC2504089. https://pubmed.ncbi.nlm.nih.gov/18751768/